
Decoding the Cognitive Test Narrative
Clinical Reality vs. Political Rhetoric

In recent years, few medical topics have sparked as much public debate as Donald Trump’s frequent references to his performance on cognitive tests. From rallies to televised interviews, the former president has repeatedly claimed to have “aced” cognitive examinations, often describing them as high-stakes, rigorous challenges involving complex mathematics and demanding mental gymnastics.
For any curious observer, this raises a fundamental question: Is there a discrepancy between the medical reality of these tests and the narrative surrounding them? By looking at what these tests actually are—and why they are used—we can separate clinical fact from political storytelling.
What Is the MoCA?
The test most frequently cited in these discussions is the Montreal Cognitive Assessment (MoCA). Developed in the mid-1990s, the MoCA is a widely used screening tool designed to detect mild cognitive impairment (MCI) or early signs of dementia. It is not an IQ test, nor is it a measure of intellectual capacity, creativity, or decision-making prowess.
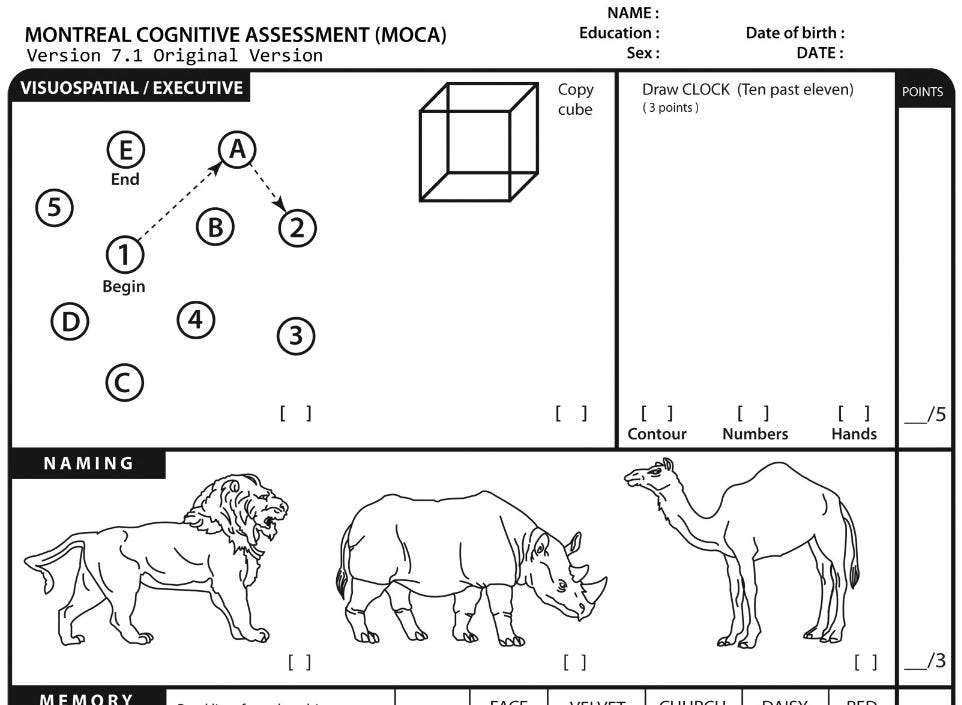
In clinical practice, the MoCA is a 10-minute snapshot. It consists of simple tasks, such as:
Memory recall: Repeating a short list of common nouns.
Visuospatial skills: Drawing a clock or copying a simple geometric shape.
Attention: Reciting digits or performing basic arithmetic (like subtracting 7 from 100).
Orientation: Stating the current date and location.
A score of 30 is the maximum. Anyone scoring 26 or above is generally considered to be in the “normal” range. The test is not a “pass/fail” academic exam; it is a clinical filter. Its purpose is to help doctors determine if a patient needs a more comprehensive, in-depth evaluation of their brain health.
The Many Faces of the MoCA
It is also important to understand that the MoCA is not a static, single document. Because the creators of the MoCA are aware that people can “practice” tests to improve their scores, they have developed several variations of the assessment to ensure accuracy.
These variations are designed to be equivalent in difficulty while changing the specific stimuli. For example, clinicians might use different “forms”—such as version 7.1, 7.2, or 7.3—which swap out the specific list of words to be memorized or the geometric figures to be copied. There are even specialized versions, such as the “MoCA-Blind” (for patients with significant visual impairments) and the “MoCA-Basic” (a simplified version designed for populations with lower literacy or education levels). By cycling through these variations, doctors ensure that a patient is being tested on their actual, current cognitive function, rather than their ability to recall a specific list of words they encountered in a check-up from a few months prior.
The Disconnect: Reality vs. Description
The most significant point of confusion lies in how these tests are described. Trump has frequently characterized the test as “very hard,” claiming it includes “very tough mathematical equations” that get progressively more difficult.
Medically speaking, this description does not align with the MoCA. The test does not contain complex or advanced mathematics. The most “difficult” arithmetic task is the aforementioned serial subtraction, which is a standard assessment for attention, not for advanced math.
The Case of “Person, Woman, Man, Camera, TV”
A clear example of this disconnect occurred in a 2020 interview, where Trump cited a specific sequence of five words—”Person, Woman, Man, Camera, TV”—as proof of the test’s difficulty. He described repeating these words back as a high-level cognitive challenge.
In clinical reality, this is simply the memory recall section of the test. The examiner reads a list of five common, unrelated nouns, and the patient is asked to repeat them back immediately and, after a short delay, recall them again. This is a basic test of short-term memory, designed to see if the brain can hold a small amount of information for a few minutes. While performing well is a good sign of cognitive health, characterizing it as a difficult intellectual feat is a fundamental misunderstanding of the test’s purpose.
When medical experts and the test’s own creator, Dr. Ziad Nasreddine, discuss the MoCA, they consistently emphasize that it is designed to be accessible. For a cognitively healthy adult, “acing” the test—that is, scoring a 30 out of 30—is the expected result, not an exceptional achievement. Describing it as a high-level test of genius is a fundamental misunderstanding of its clinical purpose.
The Question of “Practice”
A common question is whether a patient could “practice” for such a test. In psychology, there is a concept known as the “practice effect.” Because the MoCA is short and follows a consistent structure, an individual who takes it repeatedly can become familiar with the tasks.
While it is possible for someone to become better at the MoCA through repeated exposure, doing so renders the test effectively useless. The goal of a screening is to see how a person’s brain functions when presented with a novel challenge. If a patient has memorized the word list or the clock-drawing exercise, they aren’t demonstrating cognitive health; they are demonstrating memory of the test itself.
Furthermore, for a person without cognitive concerns, there is no medical reason to take a screening test multiple times in a short period. In standard care, if a patient is functioning well in their daily life, doctors do not typically require them to “prove” their cognitive health through repetitive screenings.
The Role of Narrative
If the test is basic and the results are routine, why does the narrative of “acing a very hard test” persist?
The answer likely lies in the realm of political messaging rather than medical science. By framing the MoCA as a “very hard” exam that measures high-level intelligence, a public figure can transform a standard medical check-up into a demonstration of vigor and mental strength. It turns a clinical “pass” into a political victory.
This creates a “symptom” of its own: a disconnect where the public hears a story about a genius-level intellect conquering a complex exam, while medical professionals see a standard, 10-minute routine screening used for basic health maintenance.
Personal Experience
As some of my X followers are aware of, I myself have many health issues including some neurological issues (seizures). After an exceptionally bad seizure in 2019 that essentially “erased” over a decade of learned technical knowledge, some memories, and caused some damage to the prefrontal cortex (specifically in the executive functioning area of the brain) I now get a neurological checkup every couple of years since then. This includes taking a new MoCA in addition to additional testing to track degradation.
That someone like me, with known issues, can go this long with only periodic re-testing does bring into question why someone 30+ years older requires more often testing.
The Bottom Line
When we evaluate claims about cognitive testing, it is helpful to keep a few key takeaways in mind:
Screenings are not diagnostics: The MoCA is just a quick check-up. It does not measure IQ, leadership ability, or overall wisdom.
Context matters: Medical tests are meant to be performed in a clinical environment, not used as rhetorical tools to prove one’s superiority.
Language is key: When a speaker describes a test as “hard” or involving “complex math,” they are almost certainly not talking about the same tool that doctors use to screen for dementia.
Understanding these distinctions allows us to look past the political noise. While it is certainly good news for any individual to demonstrate normal cognitive function, it is important to remember that a medical screening is a tool for health—not a trophy for intellect.